

Dr. Jack Griffin
The choices in aesthetic materials today can give us stronger cosmetic restorations than ever before. The three major indirect aesthetic choices today are zirconia, lithium disilicate, and resin-based materials. Tooth preparation and cementation techniques are critical and must be melded with the characteristics of the material chosen.
Zirconia has had a meteoric rise in popularity because of its durability and increasing aesthetic values. So if we live by the mantra of “use the most durable material that meets the minimum cosmetic need of the case” and understand those techniques, we can be conservative while giving long lasting clinical success to our patients.
You know how difficult some patients can be. They often tie your hands while dictating treatment from the perspective of what they learned on the internet. In this case, a middle-aged lady was missing an upper bicuspid and chose not to do an implant because of the danger she read about online (something about them leading to hair loss). She also didn’t want us to “cut down her teeth” because that would, of course, lead to spine problems from uneven body parts on right and left.
Zirconia has taken off because it works. Its strength allows for conservation of tooth structure and if the material is bonded correctly, even for bridges. In this case, the buccal cusp was preserved because of more than 2mm of dentin support and to increase the odds of a good aesthetic match (Fig 1). A conservative full coverage supragingival prep was done on the first molar.

Figure 1
The interproximal restorations on the premolar were made into retentive boxes for a single path of insertion. It must be stressed that the preparation is at least as important as proper bonding for maximum retention (Fig 2). A monolithic, stain only, all zirconia bridge was made by the Corr Dental Design team with excellent connectors and anatomy (Fig 3). Zirconia is not a ceramic, has no silica glass, and cannot be etched or bonded-in as a porcelain restoration would be (Fig 4). The try-in was good with no adjustments needed (Fig 5).
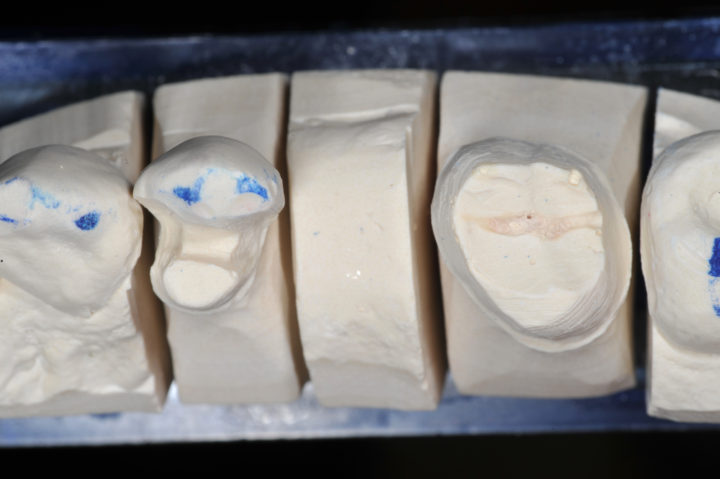
Figure 2

Figure 3

Figure 4

Figure 5
For conservative preparations, maximum long-term adhesion is needed (Fig 6). The zirconia was cleaned and a metal/zirconia primer was applied, let set for 1 minute, and air-thinned (Fig 7). The inside with properly metallic bonding should look shiny (Fig 8).

Figure 6

Figure 7

Figure 8
The teeth were isolated, pumiced, and the enamel on the bicuspid etched with 37% phosphoric acid for 20 seconds (Fig 9). After rinsing, a dual cure, universal adhesive was applied to both abutment teeth and air-thinned (Fig 10). The bicuspid was, therefore “selectively etched” and the molar, having no application of phosphoric acid, was self-etched (Fig 11). The bonding agent was air thinned and the bridge then cemented with a self-adhesive dual-cure resin cement (Fig 12).

Figure 9

Figure 10

Figure 11

Figure 12
Clean up was done with microbrushes, floss, and 204s scaler (Fig 13-15). At a six month recall, the aesthetic result was excellent with an excellent long-term prognosis because of dedication to maximum long-term adhesive techniques. Now, as long as she has no vertebral issues from the weight of the zirconia, she should be a good referral source.

Figure 13

Figure 14

Figure 15
If you have questions about my article or if you would like to send a case, please contact the Pacific Aesthetic Laboratory Group at www.pacificaestheticdentalstudio.com, Gary Vaughn, CDT, CTO (916) 786-6740, or via email [email protected].