

Dr. Michael Miyasaki
As dentists presented with aesthetic focused cases we often learn in courses how to prepare the hard and soft tissues to create the most ideal smile-evaluating proportions, contours, textures and color. That is what we learned to do in dental school, work on the teeth and gums. But what do we do with the rest of the face and associated soft tissue? In this newsletter I present to you an interesting case with an issue that we often see today-a gummy smile. Today we know one cause of a gummy smile can be early airway issues so I would hope we would try to identify that early and intervene. Some of the solutions that we might offer to our patients might be surgery to reset the bones, tissue surgery to shorten the vestibule, osseous surgery to remove bone around the teeth or just tell the patient to train their upper lip not to go up so far? With this case we will discuss how we elected to treat this issue and the treatment flow.
Our patient was very nice with two chief concerns. The first concern, discoloration of previously done veneers, and, her second, was a gummy smile. (Figure 1) It is often said that the lips are the curtain which frame the smile. Corr does a great job with the ‘painting’, but often it is up to us as clinicians to reframe the smile.

Figure 1
We discussed both of the patient’s concerns and explained that we would first handle the issue of the failing veneer restorations and then we would use Botox to limit the upper lip’s upward movement. The patient was excited about both phases of treatment.
Step one was preparing the teeth for new veneers. As the old veneers were removed we recorded the shade of the preparations, St5, so the lab could determine the degree of opacity needed in the e.Max ingots to give us the desired shade. The preparations were subgingival and we had to manage the soft tissue bleeding using Vista/Apex’s Quick Stat Gel. It is a clear hemostatic agent which I find really helps control bleeding as well as my brown ferric solutions without the staining concern. (Figure 2)

Figure 2
In this case the patient wanted a clean look without being overly bright so we selected a final shade-BL4 Cervical, BL3 Body, and light Incisal Translucency. We made the patient’s temporaries with a BL1 shade and she thought they were a little too bright (Figure 3) which I liked knowing. Many times patients don’t want to be too bright during the preparation appointment and then wish they had gone lighter after cementation so the feedback during temporization is always important to have.

Figure 3
Corr Dental Designs did a great job with the fit and aesthetics of the restorations. Using a lab that has experienced technicians who are also artist is the key to doing these types of cases (Figure 4).

Figure 4
When the patient returned for cementation we followed the protocols taught in the PAC courses, but the curing light you see here is Vista/Apex’s new PinkWave curing light that is a pink light, not blue. It used near-infrared energy to give better depth of cure with less shrinkage stress and its large head makes curing veneers and crowns go much faster. (Figure 5)

Figure 5
The patient was pleased with her new smile, which was part of the problem. She now smiled bigger (Figure 6). The solution was using Botox and here is the background on that. The primary muscles involved with lifting the upper lip when smiling are the zygomaticus major and minor which also works with the risorius, the levator labii superior, the levator anguli oris, and the levator labii superior alawque nasi muscles. They all come to a point around the base of the nose, lateral to the nostrils so that is where we placed the Botox, and very little, in fact, about 2 units on each side (Figure 7 and 8). The results were tremendous.

Figure 6
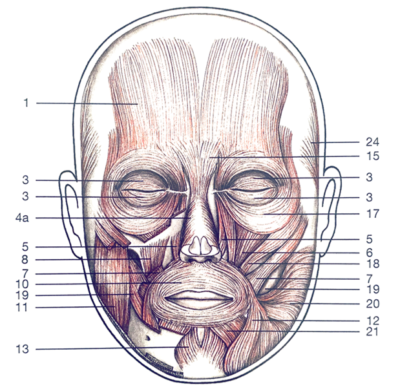
Figure 7

Figure 8
We need to understand the anatomy of the muscles involved in smiling (Figure 7). By placing just a couple units of Botox per side close to the base of the nose, lateral to the nostrils (Figure 8) we are able to affect the elevators.
Botox doesn’t work immediately, but usually takes about a week to affect the muscle movement. I explained this and suggested we re-evaluate the affects in a couple of week. Our patient shared that she noticed the Botox worked at about Day 5 and she was thrilled to see the results. She said she had been concerned about the entire procedure and had put this off for five years, and now she is kicking herself for doing so. She loves her smile (teeth) and her smile (lips) and her smile (confidence). (Figure 9) Thank you to the team at Corr Dental Designs for making us all look good.

Figure 9
If you have questions about my article or if you would like to send a case, please contact the Pacific Aesthetic Laboratory Group at www.pacificaestheticdentalstudio.com, Gary Vaughn, CDT, CTO, (888) 461-3331, or via email [email protected].