

Dr. Todd Franklin
Opportunities begin with a single desire. In our profession, the patient brings that desire allowing us to recognize and cultivate that desire. Kelly is no exception. He desired to replace a lower crown and fix the chipping on his upper front teeth. We are currently in the wax stage and will feature the finished case in a future article.
By the time you read this, we will have started to rehabilitate 22 units and give him the smile and bite of his dreams.
How does one go from wanting a few restorations to agreeing to a full mouth rehab? You keep asking questions and diving deeper into what the motivators are for the patient. Utilizing skill sets, both verbal and clinical that are taught in PAC programs, you will have an arsenal of skills that can guide the patient thru this process.
I firmly believe we as dentists talk too much in the beginning without getting the patient’s story. With experience, you will already ‘see’ what the patient truly needs and will be able to guide the patient. We should be well versed in gathering data during our initial review of our patients. The most critical pieces of the diagnosis are clear clinical photos and quality diagnostic study models. Remember that 67% of patients are visual learners and your case acceptance will dramatically rise as you incorporate visual tools in your planning sessions.
Figure 1
Looking at this case there are so many questions that arise. Why is he breaking teeth and restorations? What are the functional dynamics of his chewing habits? Is he stable in a harmonious CR/MIP bite? There must be functional stability before any cosmetic concerns can be treated. I find it beneficial for the patient to understand the damage a bad bite can cause. With study models poured in white stone I mark in red all the parafunction areas (figure 5 & 6). This identifies centric contacts and any working and balancing interferences.

Figure 2

Figure 3

Figure 4

Figure 5
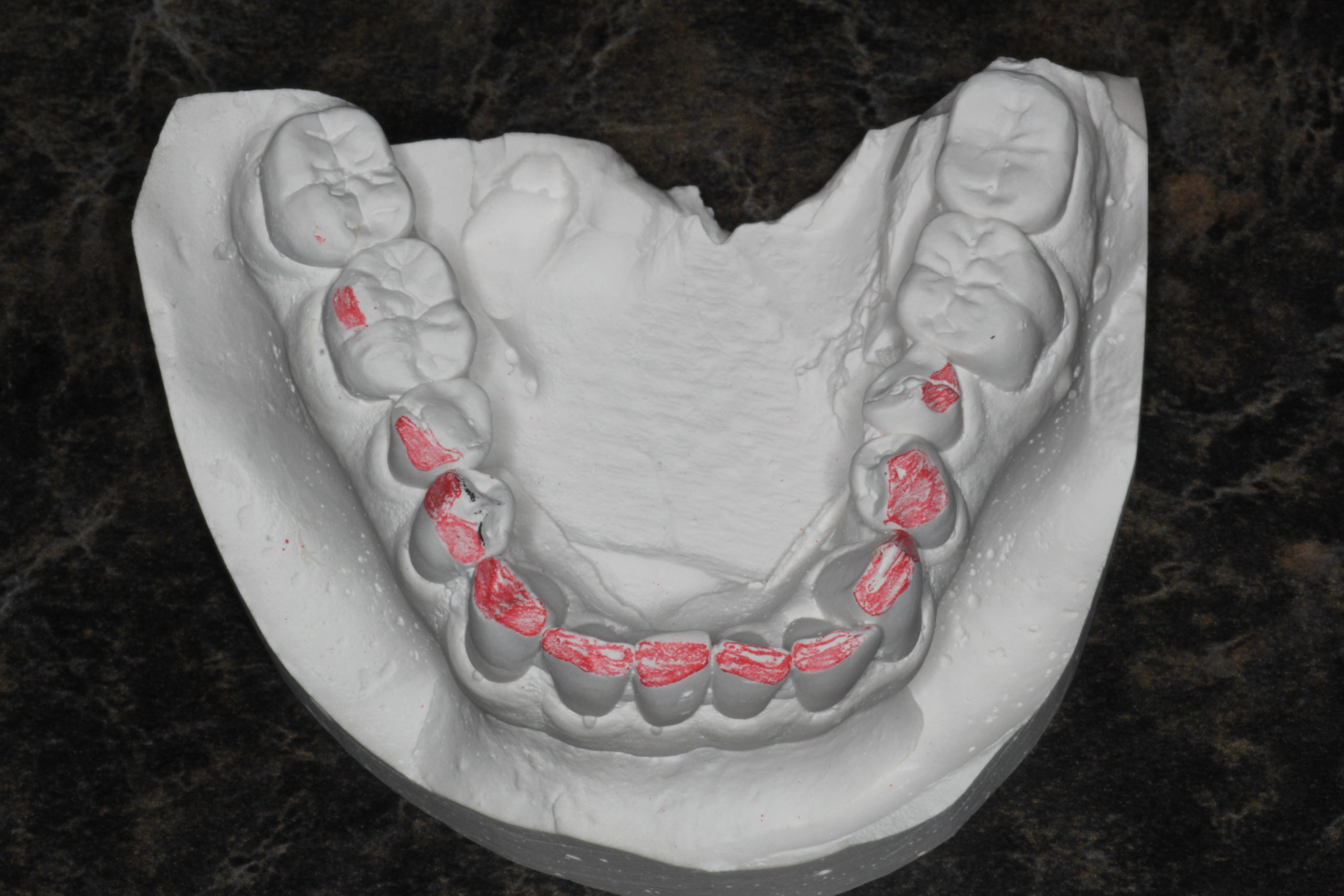
Figure 6
This is a key component in helping the patient understand the conditions of their bad bite and taking ownership of those problems. The vertical dimension is adequate for the restorative materials and we have determined that his stomatognathic system is stable and asymptomatic. We do acknowledge that he presents with a constricted envelop of function.
A definitive treatment plan was created and presented. It is important to present game plan A which is in the best interest of the patient. Kelly was ready to move forward in a single phase. That doesn’t always happen. Many times, getting the patient to accept the wax up stage allows them to ‘pre-view’ their case. Once they visually see what they could have they are ready to make the leap. Have you experienced the amazing wax-ups from the aesthetic team at Corr Dental Designs? At the end of the day, it boils down to a trust relationship.
For the treatment plan, we will be providing full coverage restorations for teeth 3-5,8,9,12,13 & 25. Onlay veneers for 20,21,28 & 29. Veneers for 6,7,10,11 making sure our centric stops are completely on porcelain. Our plan for #14 is to remove, preserve the socket thru grafting and then place an implant. We will work out any additional bite modifications beyond the wax-up in the temporaries making sure our bites allow for synchronous CR/MIP. The prep sequence will involve prepping upper and lower anteriors and capturing the anterior bite while preserving the posterior vertical dimension. With the anterior bite, we will then proceed to prep the posteriors and temporize the case.
Stay tuned! This is setting up to be a fun case to document and a life-changing event for Kelly.
If you have questions about my article or if you would like to send a case, please contact the Pacific Aesthetic Laboratory Group at www.pacificaestheticdentalstudio.com, Gary Vaughn, CDT, CTO (916) 786-6740, or via email [email protected].