

Dr. Todd Franklin
Summer is in full swing here in California and we are busy at our practices and at home. This month we revisit a complicated case from 2015.
At the PAC, we teach a Full Mouth Rehabilitation curriculum that helps you treat complicated cases. From the moment you sit down with a patient our goal is to help you simplify the process, mentor you, and help build your confidence for future cases.
Let me introduce you to Ro. She was new to us and wasn’t happy with her smile (Figures 1,2,3). After taking the time to know her story we embarked on a journey of discovery. So where do we start? As clinicians, what are all the questions that we need to have answered? At the initial meeting and seeing the amount of tooth wear present we knew we would have to look at Ro from a comprehensive view and walk her through the process.

Figure 1

Figure 2

Figure 3
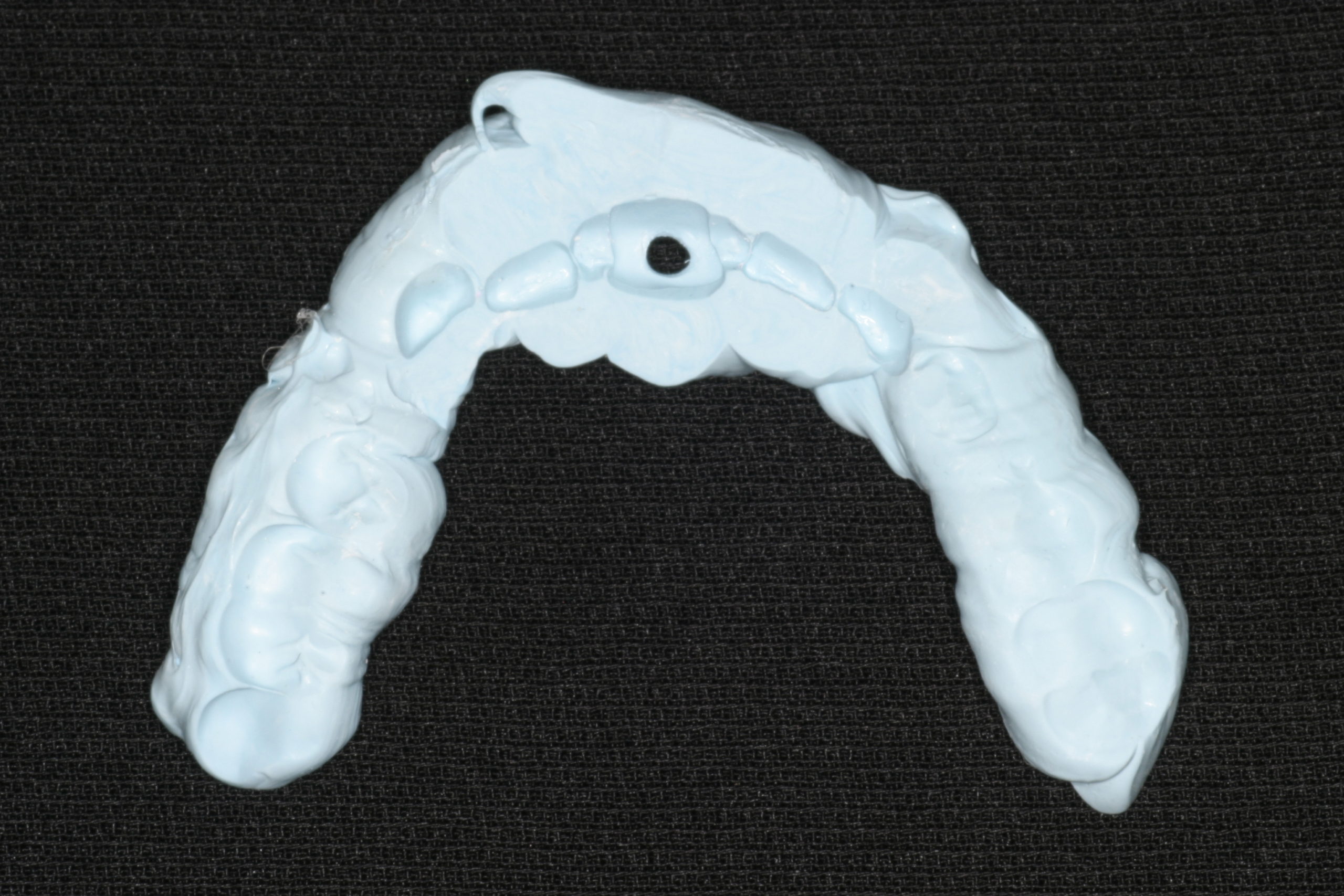
Figure 4
Once we established the need for a comprehensive records appointment, we were off. Clinical records included radiographs, a full comprehensive exam, digital photographs, PVS full-arch impressions, and a verified CR bite. Many of us may be hesitant to take on a case when we see this amount of tooth wear. Being able to predictably capture a CR record and then be able to verify the accuracy is paramount to the success of the case. In our Study Groups, we train doctors to be able to take a ‘no flash’ CR bite (Figure 4). This straightforward approach can be taken to the laboratory and mounted to verify the CR records accuracy against a first point of contact bite we have taken on the patient. At this point, we also determined the pre-op working and balancing interferences with the intent to remove them in the final reconstruction (Figures 5, 6).
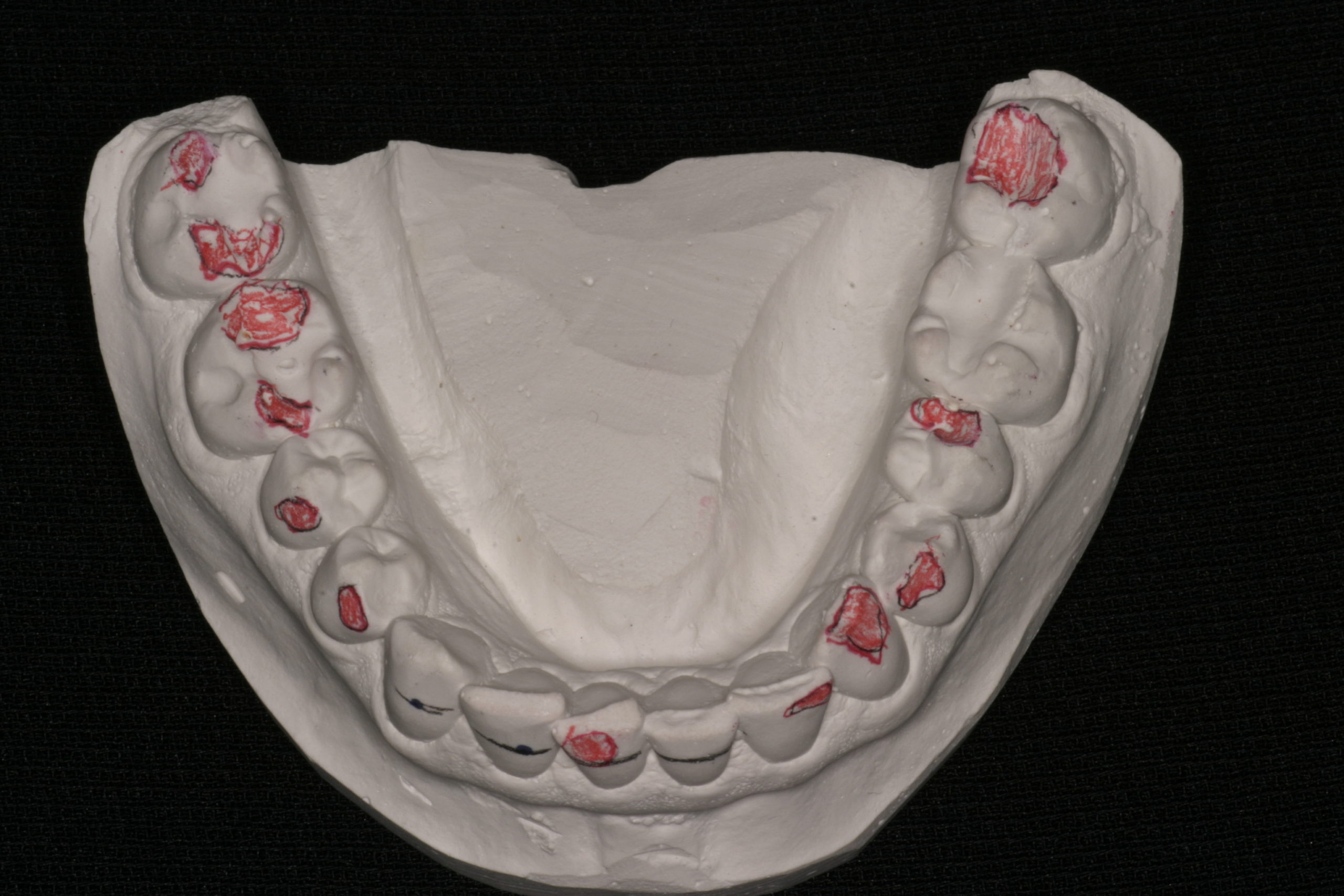
Figure 5
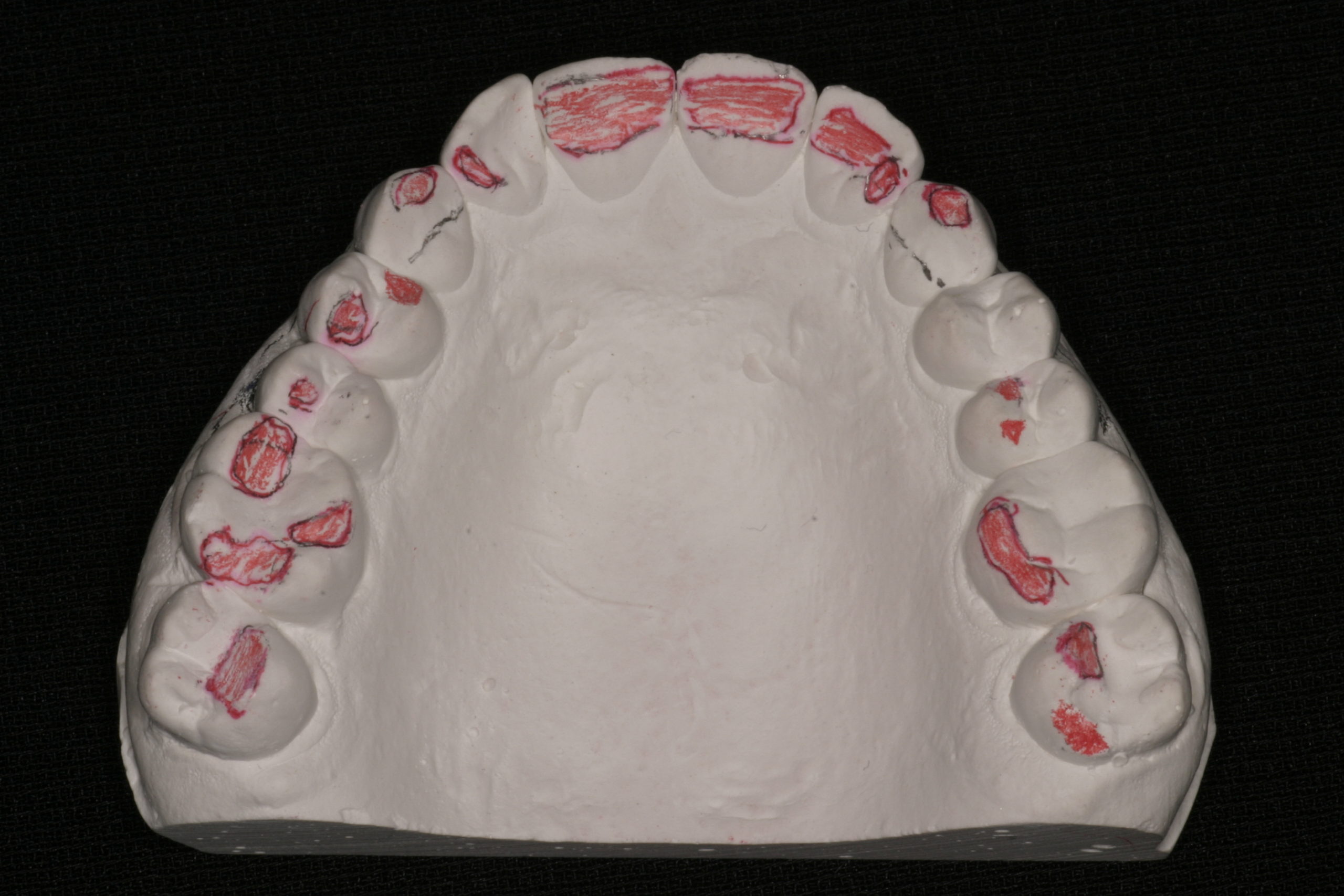
Figure 6
With an accurate mounting we can work with the laboratory and create a functional wax-up for the case. This gives the restorative dentist and the patient many options. The case can be phased for financial reasons. Transitional treatment can be used to check for stability of the new occlusal scheme. Aesthetic demands of the patient can be worked out.
Ro requested to proceed with restoring the complete dentition in a single phase. We used the functional wax-up to create the anterior architecture we desired and provided any fine-tuning needed. While maintaining an anterior stop we were able to prepare the case in a traditional manner and provide all the necessary bite records so the lab could mount the case.
The finished case achieved all the desires Ro wanted for her new smile (Figures 7,8). We were able to break the case into steps that were predictable, efficient and allowed us to find her new dental home where her bite will be safe from future damage.

Figure 7

Figure 8
We would like to thank Gary Vaughn, CDT, CTO, and the Pacific Aesthetic Laboratory Group and Corr Dental Designs for the excellent laboratory work. Having a ceramic team behind you who knows your goals makes us look good to our patients.
If you have questions about my article or if you would like to send a case, please contact the Pacific Aesthetic Laboratory Group at www.pacificaestheticdentalstudio.com, Gary Vaughn, CDT, CTO (916) 786-6740, or via email gvaughn@thePAC.org.